The Rare Diseases Act of 2002 (H.R. 4013) enacted the establishment of the Rare Diseases Clinical Research Network (RDCRN) in 2003. Since that time, the RDCRN has diligently worked toward diagnosing patients faster and helping to develop treatments for people living with rare diseases. The RDCRN currently consists of 20 different consortia, making it a network of networks with sites around the world. Each consortium studies at least three different rare diseases and includes scientists, clinicians, patients, and advocates collaborating to advance rare disease research.
The RDCRN is supported by NIH grants. Every five years, the NIH requests research applications that are reviewed by scientists and patient advocacy group members. The applications that score well and fit the mission of one or more of the participating NIH institutes are funded.
One of the primary focuses of the RDCRN is clinical trial readiness—knowing who to treat, when to treat, and how to treat. By conducting natural history studies, each group learns more about the development and outcomes of rare diseases, taking some of the risk out of clinical trials.
To date, the RDCRN has published more than 2,500 manuscripts, with topics ranging from natural history studies and case reports to practice guidelines and clinical trials. Additionally, findings from the RDCRN have contributed to the approval of 10 treatments for rare diseases by the US Food and Drug Administration (FDA).
In a new publication in the journal Therapeutic Advances in Rare Disease, RDCRN Scientific Program Manager Joanne M. Lumsden, PhD, and Program Director Tiina K. Urv, PhD, provide an overview of the RDCRN since it was first established 20 years ago. Here, they share what they’ve learned about the network’s productivity and influence, as well as future goals.
Why is it important to understand and document the progress of the RDCRN?
Dr. Lumsden: We’re all scientists, and it's important to evaluate the progress of the RDCRN and document its success. Doing this allows us to be more agile when facing new challenges and be better equipped to seize new opportunities. Moreover, as NIH funding for scientific research becomes increasingly competitive, providing a quantitative and informed description of our research productivity and influence is crucial. This will enable the RDCRN to continue making a significant impact on the rare disease community.
Why did you decide to focus on the topic of clinical trial readiness?
Dr. Urv: Overall, our focus on clinical trial readiness is all about developing treatments more efficiently and effectively. Developing treatments for rare diseases is a challenging process. The current process is slow, expensive, and risky. By being well prepared for potential treatments, we can lessen some of the risk and move quickly into new clinical trials and effectively evaluate treatments. This includes natural history studies, strong networks of clinicians experienced in conducting clinical trials, and input from patient advocacy groups. And, by identifying biomarkers as well as sensitive and specific outcome measures, we can accurately assess targeted treatments.
Conducting rigorous science and having high quality data is also critical. This data can be replicated and shared and is valuable to industry and regulators when it comes time to conduct clinical trials.
Were there any discoveries or achievements that stood out to you most?
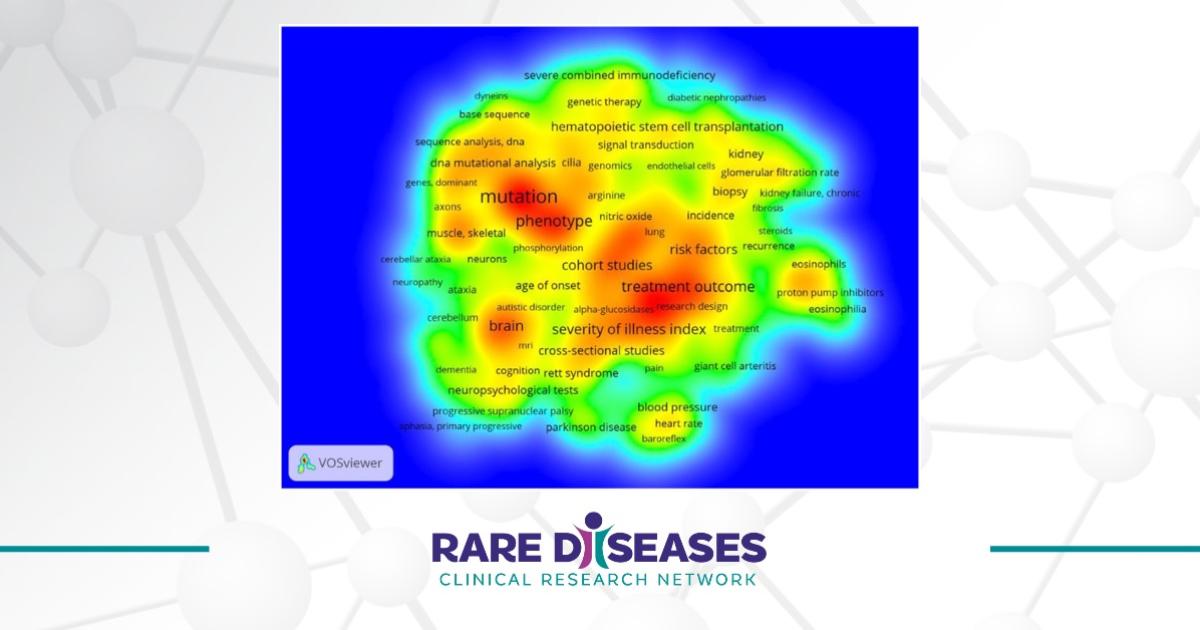
Dr. Lumsden: Identifying specific examples is difficult since there are many achievements, and everyone has excelled and contributed. Part of the analysis for the paper was constructing network diagrams of RDCRN individuals, institutions, and countries. These provide a wonderful visual representation of the significant growth and influence of the network over the past twenty years.
How have you personally witnessed the RDCRN’s impact on the rare disease community?
Dr. Urv: One of the key aspects of the RDCRN is the relationships that are established between the research scientists and the patient advocacy groups. It's a unique experience that allows for mutual learning and growth, benefiting everyone involved. Our intent is to establish a research community where every member is valued.
How can the RDCRN improve in the coming years?
Dr. Urv: As we reflect on the success of the longstanding RDCRN program, it's crucial that we look towards the future and anticipate the challenges that may lie ahead. To achieve this, we must prioritize enhancing diversity, equity, inclusion, and accessibility for diagnosis and treatment. We also need to focus on building robust data-sharing systems and leveraging artificial intelligence and machine learning to their full potential. Lastly, we should consider groups of conditions together, rather than focusing on one rare disease at a time.
What excites you most about the future of the RDCRN?
Dr. Lumsden: A significant challenge is the sheer number of rare diseases that exist and that need treatments. At the end of the current cycle, several groups will graduate from the RDCRN after three cycles of support. We’re excited to follow their progress and to work with new groups that will have the opportunity to benefit from participating in the RDCRN.
Dr. Urv: The sheer potential of the new science coming down the road; this includes artificial intelligence, gene editing, new technologies… if we work collaboratively, the sky is the limit.
The Rare Diseases Clinical Research Network (RDCRN) is funded by the National Institutes of Health (NIH) and led by the National Center for Advancing Translational Sciences (NCATS) through its Division of Rare Diseases Research Innovation (DRDRI).